ECR 2015 / C-0247
Autoimmune Pancreatitis – What every Radiologist needs to know now
This poster is published under an open license. Please read the disclaimer for further details.
Congress:
ECR 2015
Poster Number:
C-0247
Type:
Educational Exhibit
Keywords:
Pancreas, CT, Education, Cancer
Authors:
G. Miles, T. Adlan, F. Wotton, S. Jackson; Plymouth/UK
DOI:
10.1594/ecr2015/C-0247
 Autoimmune pancreatitis: instrumental diagnosis. Journal of pancreas online 28-30")
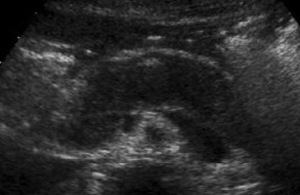
Fig. 16:
US image of 45 year old male with AIP showing diffuse enlargement of the...

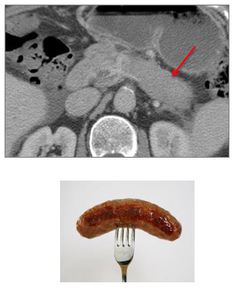
Fig. 17:
CT demonstrating "Sausage-shaped" pancreas

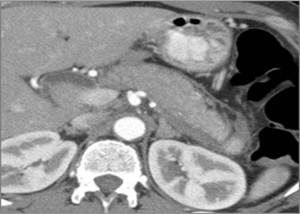
Fig. 18:
CECT demonstrating thickening of the pancreatic envelope

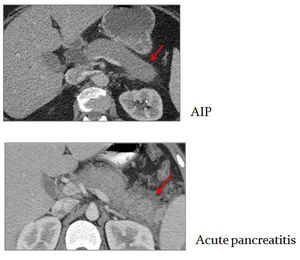
Fig. 19:
CECT appearances of AIP vs Acute pancreatitis fat stranding

Fig. 20:
Pre-, pancreatic parenchymal and delayed phase CECT demonstrating delayed...

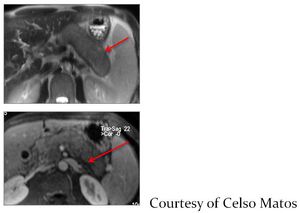
Fig. 21:
MRI demonstrating inflammatory peripancreatic "capsule"

Fig. 22:
MR findings of pancreatic ductal AIP
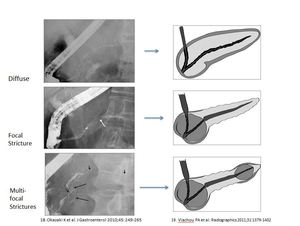
 J Gastroenterol 45:249-65 and Vlachou PA et al. (2011) Radiographics 31:1379-1402")
Fig. 23:
Spectrum of AIP ductal involvement on ERP with accompanying schematic...

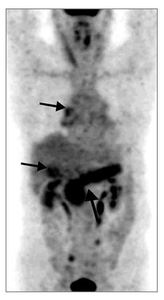
Fig. 24:
PET/CT demonstrating FDG uptake in organs involved in IgG4-related disease

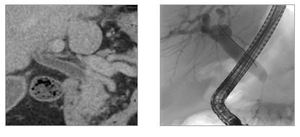
Fig. 25:
CBD enhancement on CECT and intrapancreatic biliary duct stricture on ERCP

Fig. 26:
Multi focal strictures of the biliary tree in IgG4-related sclerosing...
 Extrapancreatic findings of IgG4-related disease. Clin radiol 69:209-18")
Fig. 27:
MRI: IgG4-related sclerosing cholangitis
CT: Thickened enhancing gallbladder...

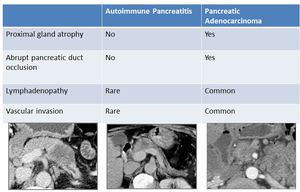
Fig. 28:
Features to differentiate focal AIP from pancreatic cancer
 References: Kamisawa et al. (2010) Differentiation of autoimmune pancreatitis from pancreatic cancer by diffusion weighted MRI. Am J Gastroenterol 105:1870-5")
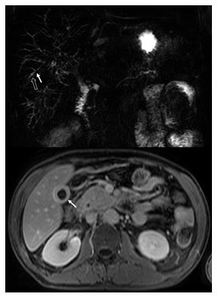
Fig. 29:
DWI and ADC map images demonstrating restricted diffusion of AIP within distal...

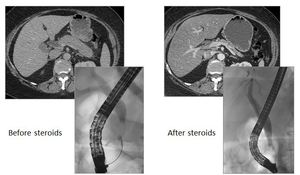
Fig. 30:
CT/ERCP pictures of AIP pre and post steroid treatment demonstrating resolution...
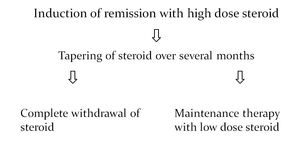
 Standard steroid treatment for autoimmune pancreatitis. Gut 58: 1504-7")
Fig. 31:
Treatment algorithm for Type 1 AIP: Initial attack
 Standard steroid treatment for autoimmune pancreatitis. Gut 58:1504-7")
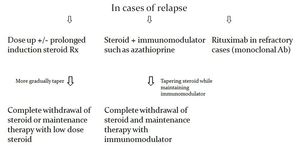
Fig. 32:
Treatment algorithm for Type 1 AIP: Relapse